Rectal Prolapse
Background
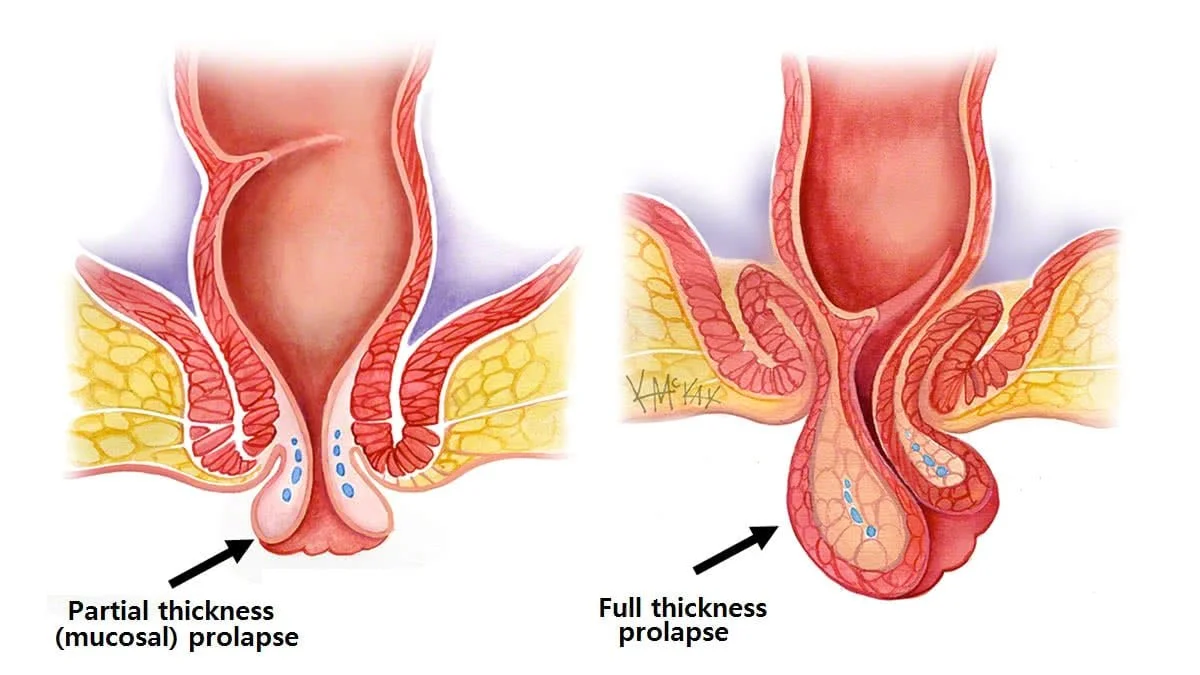
Rectal prolapse occurs when the rectum, the final section of the large intestine, slips or protrudes through the anus. It can be partial, involving the inner lining only, or complete, where the entire rectal wall extends outside.
Causes
Rectal prolapse often is often caused by a combination of risk factors and there is usually not a specific single cause. Risk factors include chronic constipation, straining during bowel movements, weakened pelvic floor muscles (often due to pregnancy and childbirth), ageing, and occasionally other more rare conditions including connective tissue disorders.
Symptoms and Diagnosis
Symptoms often include a visible protrusion, discomfort, faecal incontinence, and bleeding. Occasionally it can be difficult for patients and their doctors to differentiate between haemorrhoidal prolapse and full rectal prolapse. Diagnosis typically involves physical examination by a colorectal surgeon and a colonoscopy or flexible sigmoidoscopy combined with an examination whilst anaesthetised. Sometimes special imaging tests are required (defecating proctography).
Treatment
Non surgical
The majority of cases of rectal prolapse will require surgery to fix them. Non surgical management can help control symptoms and reduce the risk of recurrence post surgery.
Dietary Modifications: High-fibre diets and adequate fluid intake to prevent constipation and straining during bowel movements.
Bowel Regimen: Use of stool softeners or laxatives to maintain soft stools and reduce straining.
Pelvic Floor Exercises: Strengthening the pelvic floor muscles (through specialist pelvic floor physio can help.
Biofeedback Therapy: A specialised physiotherapy to improve control over pelvic floor muscles and rectal sensation.
Manual Reduction: Gentle manual pressure to reposition the prolapsed rectum if it becomes externalised.
surgery
Surgery for rectal prolapse can be divided into 2 broad approaches:
Perineal Procedures: Operations done from “below”, avoiding any abdominal incisions. These are usually very low risk, but have a high recurrence rate. They are often reserved for very frail or elderly patients. The most common example is a Delorme’s Procedure.
Abdominal Procedures: These are operations performed with keyhole or open incisions through the abdomen. They are usually more successful then perineal procedures and have a lower recurrence rate. The commonest would be a Ventral Rectopexy.